
How do we balance the risks of vaccines and the benefits of our population being vaccinated? How do we balance the individual risks and benefits and the collective risks and benefits?
My view is that we should be asking people to take remote individual risks (such as vaccination complications) for the collective benefit (ultimately population immunity against Covid19). We need to have this conversation as a country, as vaccinations and border opening will involve difficult tradeoffs between individuals and society as a whole.
The best examination of individual risks and benefits of vaccination I have seen is in the completely open review in the US by the Advisory Committee on Immunization Practices (ACIP) of the Johnson & Johnson vaccine’s clotting risks and whether it should continue to be used in the US. The hearing was streamed, in an impressive example of open and transparent government. Statnews has the full story here.
ACIP, as the panel is known, found that Johnson & Johnson’s vaccine is safe for the vast majority of people and is saving lives. Even for the age group that appears at highest risk — women aged 30 to 39 — the risk from Covid is greater than the risk of developing TTS after getting the J&J vaccine, CDC scientists told the committee.
This diagram was a key part of the considerations for the committee.
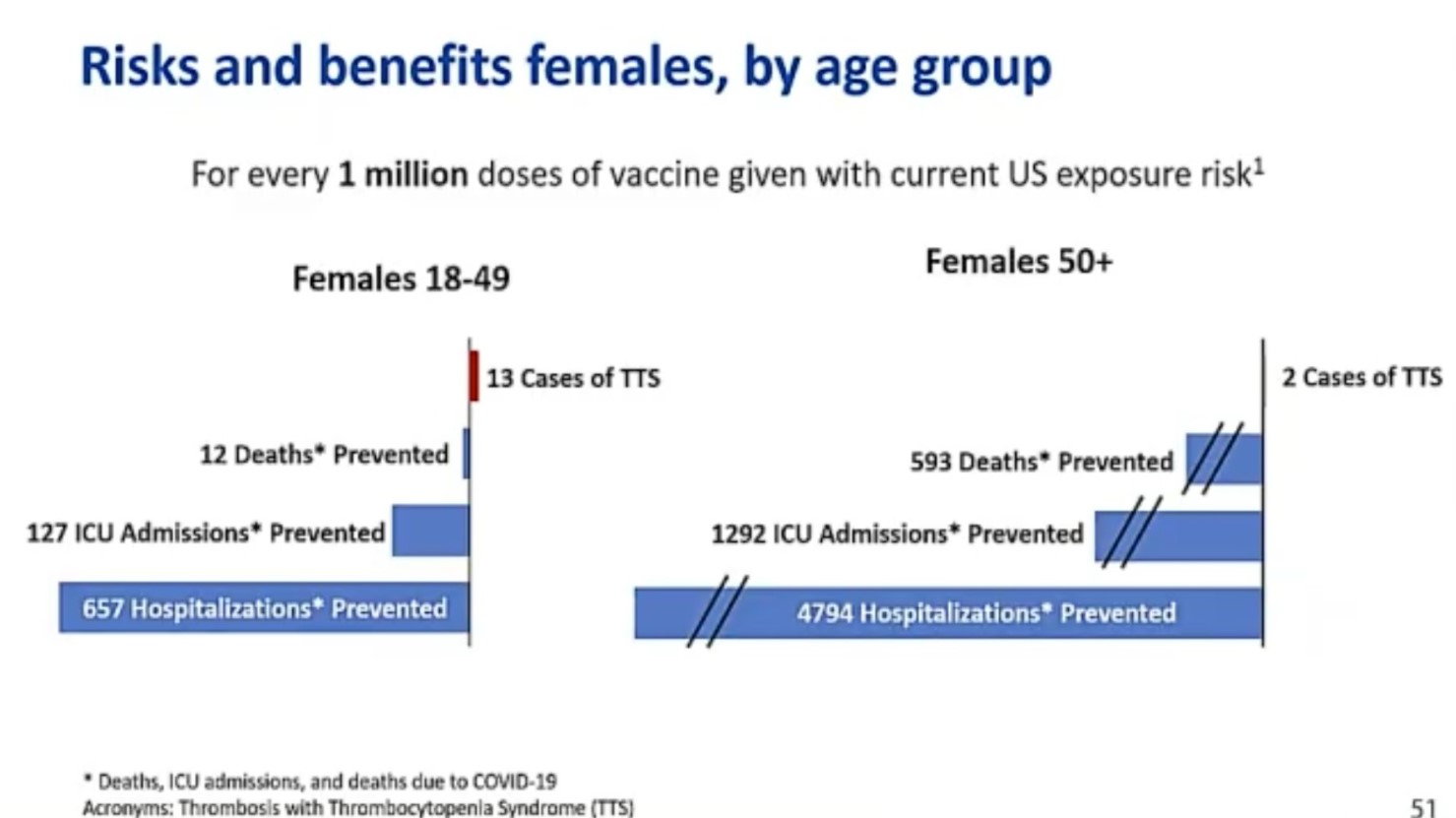
It shows that ACIP considered the current risks of Covid compared with the current risks (as known) from the vaccine. For women under 50, the tradeoffs were quite close, and for women over 50, at the current prevalence of Covid19 in the US, the vaccine was massively beneficial compared with the risk of Covid19.
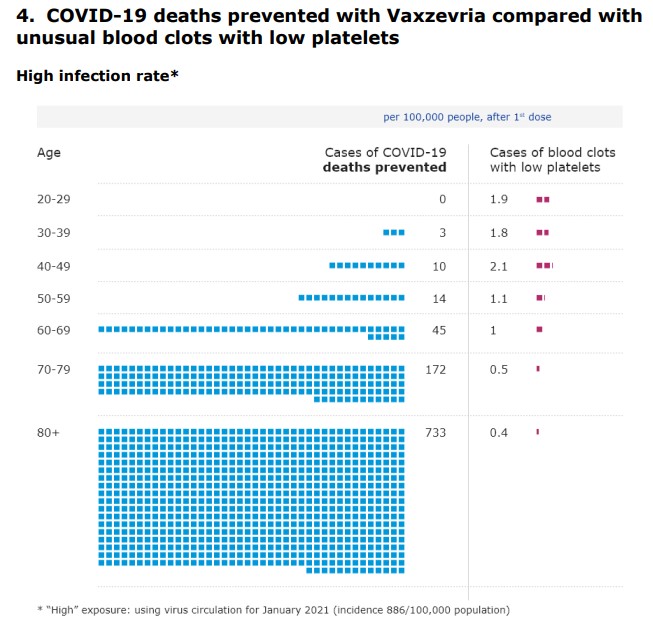
A similar piece of visualisation was done by the European Medicines Agency for Astra Zeneca. Again, this graph shows the deaths caused by Covid (under a high infection rate scenario based on Europe in early 2021) compared with the deaths caused by the unusual blood clot combination by age.
But this is comparing the risks and benefits of vaccination for an individual. And the only benefits considered are the benefits of not becoming ill, in a situation where there is a lot of Covid19 around. How should we think about these risks and benefits in a situation like Australia and New Zealand, where there is very little Covid19 around?
One way is to continue thinking just about the individual being vaccinated, and the risks in our current Covid19 prevalence. And that quickly leads to a situation where the risk of vaccination is worse than the risk of the disease for quite a lot of people.
But that ignores quite a lot of other benefits, which haven’t been taken into account, particularly as it becomes increasingly likely that vaccines stop transmission, and hence will eventually create population immunity if enough people are vaccinated:
- For individuals, the benefit of being able to participate more fully in normal life – going out, seeing friends and family etc
- For those who can’t be vaccinated (especially for medical reasons) they will also be less likely to become ill with Covid19
- For the whole of a Covid19 infected society, the more people are vaccinated the more normal life can resume
- schools/universities reopening
- seeing friends and family
- restaurants/theatre/sport etc can reopen
- economic benefits of all of these
- And for countries with closed internal or external borders (such as Australia and New Zealand, but many others), reopening the borders would be a huge benefit both economically but to all those people who have friends and family overseas.
Ultimately the tradeoffs between individual risks and society benefits are those for a society to make. But they are not easy. And they are much harder when the risks are clear, but the benefits are less clear.
We implicitly make these trade offs in choices we make as a society. For example:
- road safety – individuals choose to drive, despite the (small but non zero) risk of death and government chooses how much money to spend on improving safety, and how much to enforce safety measures like random breath testing, seat belts etc.
- medicine – in funding our public health system, we as a society choose how much money to spend on treatments which are high cost but low (but not zero) effectiveness such as new drug treatments for cancers, or how much money to spend on funding health professionals such as doctors and nurses being available for all
- emergency services – how well we fund and the risks we ask our emergency services personnel (such as firefighters) to take on behalf of others are trade offs of risk and reward between individuals and wider society.
In Australia, in 2020, there were 1,108 deaths on the road. That’s 4.31 deaths per 100,000 population, a proportion that has been steadily improving for many years. It is at least twice as high as the death rate from Astra Zeneca vaccinations from platelets. But for the individual driving on the road, there is a benefit – we get to go somewhere. And the risk doesn’t seem as immediate as injecting something into our arms and waiting to get sick.
This is very similar to the argument that was made in very places at the beginning of the pandemic, that we should just open up our economy to Covid19, and let it rip as the individual risks were worth it for the country as a whole. And I fundamentally disagreed with that argument. So what is the difference? It’s a level of risk. For the population as a whole, mortality rates from Covid19 are around 1% – ie if everyone in the population is infected with Covid19, approximately 1% will probably die. This is very different by age, (this study has a lot of detail), but even at young ages, it is serious. The risk of serious harm from blood clots from Astra Zeneca is at most 1.1 per 100,000, so one hundred times lower than the risks arising from Covid19 infection.
Ultimately there is no right answer to what is an acceptable (random) risk to individual people in a population for a benefit to the country as a whole. For me, someone who is currently eligible for AstraZeneca vaccine, 1 in 100,000 is acceptable. It is lower than risks I take in my daily life on a regular basis.
This is a conversation we need to have. It isn’t enough to say that if the individual risk is lower than the individual benefit, we shouldn’t ask people to take it. The collective benefit from vaccination is real. I would be willing to take a small, non zero risk of death for the benefit of all Australians. I’d like to think others would feel the same.
Links
Peter Doherty (australian virologist, Nobel Prize winner and National Treasure) does a weekly blog on all things Covid. In this post he’s talking about vaccines, side effects, and efficacy:
From that overseas experience, we have also learned that there are a few categories of people who may be at risk of severe side effects. This came through first for the PfizerBioNTech (BP) mRNA vaccine with the demonstration that people who are highly allergic (EpiPen users) could be at risk of anaphylaxis (#43). With the AstraZeneca (Az) vaccine, the concerns raised in Europe re blood clotting seem to be narrowing down to, especially, women under 55 with a history of DIC (disseminated intravascular coagulation) or CVST (cerebral venous sinus thrombosis), both rare conditions. It’s still early days but, by now, any clinic administering the vaccine will presumably be well aware of these suggestive findings.
What do we know about the immune responses resulting from the intramuscular (IM) injection of the BP and AZ vaccines? The information I’ve been able to access so far is a bit fragmentary but, especially after the second booster shot, both seem to be inducing protective, neutralising antibody responses.
And there have been a few studies into long covid, now that there is more data available from some people being sick for 12 months or more. This one (mostly US patients) looks at neurological and psychiatric outcomes compared with control patients diagnosed with flu or other respiratory diseases – Covid19 was substantially higher than other respiratory diseases to leave patients with serious neurological or psychiatric diagnoses:
Among 236 379 patients diagnosed with COVID-19, the estimated incidence of a neurological or psychiatric diagnosis in the following 6 months was 33·62% (95% CI 33·17–34·07), with 12·84% (12·36–13·33) receiving their first such diagnosis… Most diagnostic categories were more common in patients who had COVID-19 than in those who had influenza (hazard ratio [HR] 1·44, 95% CI 1·40–1·47, for any diagnosis; 1·78, 1·68–1·89, for any first diagnosis) and those who had other respiratory tract infections (1·16, 1·14–1·17, for any diagnosis; 1·32, 1·27–1·36, for any first diagnosis). As with incidences, HRs were higher in patients who had more severe COVID-19 (eg, those admitted to ITU compared with those who were not: 1·58, 1·50–1·67, for any diagnosis; 2·87, 2·45–3·35, for any first diagnosis). Results were robust to various sensitivity analyses and benchmarking against the four additional index health events.
And this one (UK patients) looks at organ specific impairment risks after hospital admissions:
Individuals discharged from hospital following COVID-19 face elevated rates of multi-organ dysfunction compared with background levels, and the increase in risk is neither confined to the elderly nor uniform across ethnicities. The diagnosis, treatment and prevention of Post Covid Syndrome (PCS) require integrated rather than organ- or disease-specific approaches. Urgent research is required to establish risk factors for PCS.
Life Glimpses
It’s been a while since I last posted and despite the occasional outbreak in Australia, Sydney is feeling even more normal (even with two community cases in the last few days). A few activities for me since my last post that would have been astonishing a year ago when we were in lockdown:
- An in person conference and dinner in Sydney with more than 100 people
- A business trip to Melbourne and dinner at one of the many hipster restaurants in the centre
- Getting into a bus with every seat filled (a few masks, but not many)
- A buffet lunch at a conference
I’m inching closer to getting vaccinated (and my mother now has her first dose) but I did the next best thing and had my annual flu shot.
Bit of Beauty
This juxtaposition of old (a classic Georgian building) and new struck me on a recent bike ride through Sydney.

For some weeks now, I’ve been pondering what the impetus is for those aged over 50 to get the AZ vaccine now, as opposed to waiting until later in the year to get a different (safer?) vaccine. With last night’s budget assuming international borders will not open for another year approx, I fail to see why the over 50s (other than those working in quarantine and their families), and particularly those aged 50-70, would risk getting AZ now. While yes, the risk of blood clots is very low, it seems the risk of covid is even lower given that we have almost zero community transmission, and state govts who are now very good at containing any small outbreaks. And the covid risk isnt going to increase substantially for another year. As someone who is very much a pro-vaxxer, and I am thinking about not getting vaccinated yet, what does this say about the success of our rollout? Our Govt needs to set clear targets and timeframes so that people will be encouraged to get the vaccine, and to get it now.
But, the faster we are all vaccinated, the faster we can return to “global life”. i would suggest that if we can get to a high proportion vaccinated earlier then borders will open (but with zero inside knowledge!). We need to be conscious that the rest of the (western) world is potentially going to open up very quickly in the latter part of this year and we risk being held in “gilded cage”. this will have devastating longer term consequences on a number of our industries, which have already been decimated during this crisis. there are problems with all the vaccines, it’s just that AZ’s are more well promulgated.
I completely agree. Which is why we need clear targets for numbers vaccinated and for the public to know the consequences of hitting (or not) those targets.
I agree with you both – and increasingly our economy is suffering from lack of people coming in – interesting article in the AFR today focusing on overseas expats deciding to leave as they won’t be able to go home (with right of return) for a long time. But normal life is going to involve more sickness from Covid than currently, and some (not zero) complications from vaccines, which we need to start talking about why it is worth while and what an acceptable level might be.
Somewhere, the message got lost. When this all started and the herd immunity debate was raging, my recollection is that mass vaccination was generally accepted as the target.
The people in countries with major outbreaks and consequent disruption seem to have embraced vaccination, yet we see it as carrying too great a risk for too little benefit.
Those who want to go overseas or welcome overseas visitors (to be reunited with family, explore the world or rebuild inbound travel business, etc) are surely strongly in favour of vaccination, since there is no plausible alternative. But we may be very much in the minority.
What is the path back from here? How does the messaging need to change?