
Today’s Insight
This great post on linkedin talks about the difficulty of calculating a case fatality rate for Covid19.
A case fatality rate is the probability that someone will die if they are infected with Covid19. And to calculate the rate you need a numerator – a number of deaths, and a denominator – a number of cases.
Let’s start with the number of cases. In order to get a true number of cases, you need to have found all the positive cases. It seems reasonably well established that some people get very mild symptoms, or even none at all. Some people get symptoms that mean they are lying in bed for a week. And some are sick enough to be in hospital, even in intensive care. And sadly, some die. In some health systems (eg New York right now), testing only happens if you are sick enough to go to hospital. So most of the cases aren’t even counted. But even if they are, they are still in progress. There are people who have tested positive, who are alive, who will eventually die of Covid19. We hope not very many, but there are some.
So the number of deaths is also hard to estimate. Both because they haven’t yet all occurred, and because (see my post from yesterday) they aren’t always counted, as the death might have occurred before testing could take place.
This article in the Lancet talks about the many different estimates that have been out there, and uses the Diamond Princess (the ship that was quarantined off Japan in February) as the best laboratory, and calculates a case fatality rate of just under 1%, since the whole ship was tested, so they can be reasonably comfortable they identified all the cases.
A unique situation has arisen for quite an accurate estimate of the CFR of COVID-19. Among individuals onboard the Diamond Princess cruise ship, data on the denominator are fairly robust. The outbreak of COVID-19 led passengers to be quarantined between Jan 20, and Feb 29, 2020. This scenario provided a population living in a defined territory without most other confounders, such as imported cases, defaulters of screening, or lack of testing capability. 3711 passengers and crew were onboard, of whom 705 became sick and tested positive for COVID-19 and seven died,6 giving a CFR of 0·99%. If the passengers onboard were generally of an older age, the CFR in a healthy, younger population could be lower.7
That rate is a lower rate than most rates I have read. So far, I’m using the estimates made by the Imperial College London study I linked to previously. The other point to note here is that the rate is very very different by age. The older you are, the worse the fatality rate. So the age distribution of a country can make a big difference to the overall fatality rate for Covid 19.
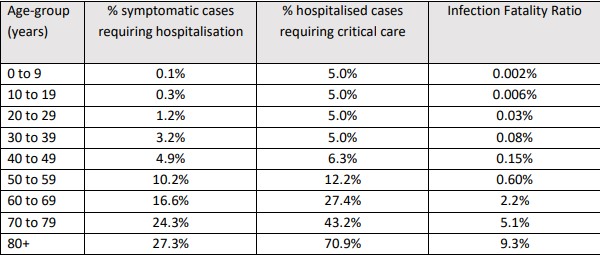
If we translate these rates to the whole population (ie every person in Australia is infected with the diseas, which no expert expects, even with no social distancing), then this would be a population mortality rate of just over 1% based on the age distribution of the Australian population.
And for those who think 1% doesn’t sound too bad, if the whole population was infected, that would be around 250,000 deaths in Australia that wouldn’t otherwise occur.
Case fatality rates are very difficult to estimate, until the epidemic/pandemic has been around for a while. So we don’t really know. But hopefully this analysis gives you an insight as to why it is so difficult.
The World in data has a whole lot more here, if you want some more data from different places.
Quick reader question
And for my statistical readers, I found a statistic today that 50% of New York tests were positive, but only 2% of tests in Australia are positive (link to yet another great source of statistics put together by a volunteer). My son and I were trying to figure out whether we could use those statistics to infer anything about how many positive cases there were in the community that hadn’t been identified. Any ideas from my readers?
Today’s link
I’m cheating here a bit, my best link today is another good source of Covid19 statistics in Australia – this one also shows how many people are in intensive care (although I don’t know the source of those statistics).
The other fascinating link is to the NZ study that drove the Level 4 lockdown in New Zealand. It is apparently similar to modelling done in Australia (which hasn’t yet been released) and makes the case for the full lockdown that New Zealand is now in the middle of. The Sydney University study a few days ago makes a similar case. If enough people fully isolate, then the virus will go through the population until there is no one infectious left (even people without symptoms).
Life Glimpses
NSW is now in much more severe lockdown. The rules are still complicated (and incredibly, the schools are still open), but there are five main reasons you can leave the house:
- Work, if a person can’t work from home
- School or an educational institution
- Shops for food and other essential items
- Get medical care
- Exercise, but only if the exercise is done alone or with one other person
Those reasons don’t count visiting your extended family, so my mother (who lives five minutes away) came around for dinner for the last time for a while last night. She normally comes around twice a week for dinner. Apparently we are allowed to visit her one at a time, so we’ll be doing her shopping for her.
Bit of Beauty
Today’s bit of beauty comes from the sculpture walk at Lavender Bay. We couldn’t decide whether a 6 kilometre walk was too far for the rules, but proper social distancing was observed.

Thank you Jennifer.
Did you get my comment, did I post it already, if not please keep writing and do to Lavender Bay again
Love Marta
The more sure you are that a person is likely to be covid-19 infected prior to testing, the higher the positive rate. Conversely, the wider you test, then the lower the positive rate. So the percentage of the Australian community currently infected is likely to be less than the current percentage positive rate.
I’d wonder whether it is possible to extrapolate from current ICU bed occupancy to the infection rate, but I suspect the very high proportion of overseas originated infections makes that meaningless at the current time.
I’d be interested in your views on the R0. My own thoughts on it are that, with the current estimates of 2 to 3, an average ‘infected’ is likely to pass it on to a small number of people and those would be the ones spending the most time with them. Super spreaders (whether people, locations such as nursing homes and hospitals, or events such as the Mt Vernon Choir practice) would push that average up, but I don’t know whether there’s anything breaks an R0 down in this manner
Measure declared case in any jurisdiction with ratio of new cases reported; then compare that number between jurisdictions; modified for age profile (mean average age) to get reporting rate; hence under reporting.
Thanks Jennifer. The interesting question is which is the best strategy to adopt – Isolate Australia and try to extinguish the virus (lengthy isolation) …vs control the spread over a very extended period and hope that builds immunity across the community. I’m sure that there is much being written on this topic – it’s a risk management topic with probabilities and trade-offs which are fascinating to reflect on.