
Here in Australia, Pfizer and Astra Zeneca vaccines have been approved and are being rolled out. So how effectively they will create herd immunity? Early indications are the Pfizer vaccine has a good chance of getting a population to herd immunity, but the Astra Zeneca vaccine is much less likely to get us there.
Let’s look at the what we know about vaccine efficacy so far. This illustration shows some possible vaccine effects. A reminder that there are two things a vaccine will do – they will stop or massively reduce disease (Covid19), and they will also stop asymptomatic infection with the virus (SarsCov2). Both Pfizer and Astra Zeneca are very effective at stopping and/or massively reducing the symptoms of Covid19. But for the roughly half of all SarsCov2 infections which are asymptomatic, but can still spread the disease, what do the vaccines do?
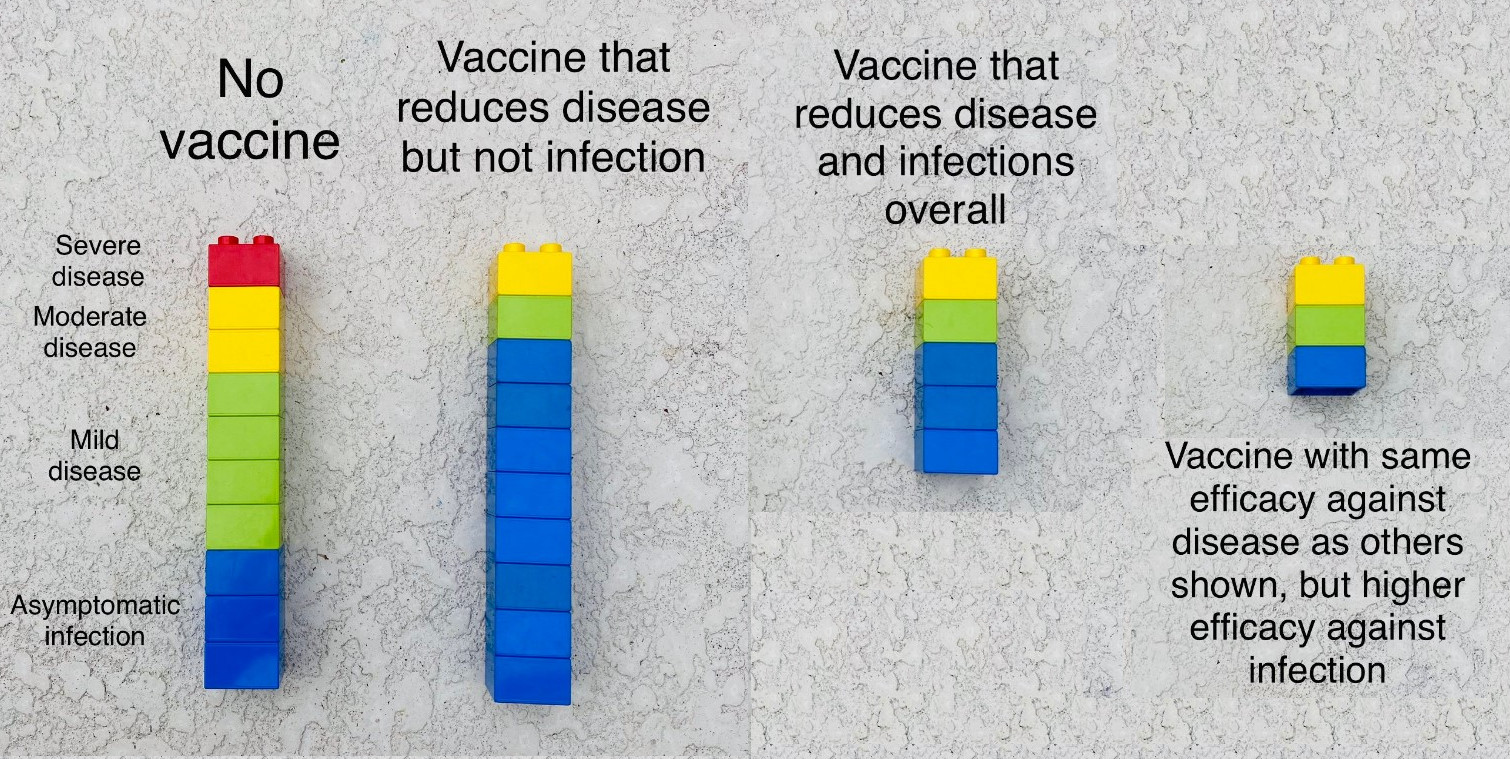
Source: Natalie Dean, Assistant Professor of Biostatistics at University of Florida
There are three broad ways a vaccine could be affecting asymptomatic infections shown above, with the third one being the best:
- All symptomatic infections become asymptomatic
- The number of asymptomatic infections stay the same, but a high proportion of symptomatic infections disappear entirely after immunisation.
- The asymptomatic infections also reduce substantially, perhaps in line with the reduction in symptomatic infections.
So what do we know about the various vaccine’s efficacy against all infections?
To achieve approval, all the vaccines went through a process of testing their efficacy. Random people received the vaccine or a placebo. And then researchers checked how many people in each group ended up with symptomatic Covid19. But no initial test looked closely at asymptomatic Covid19. Now that many people have been vaccinated around the world, data is starting to emerge about asymptomatic infections too.
Pfizer
The best estimate of Pfizer efficacy against symptomatic infection is 95%. This new study, about Pfizer, from the UK, suggests that one shot of Pfizer will reduce asymptomatic infections four fold – or 80% efficacy for asymptomatic cases:
The study, which has yet to be peer reviewed, found that 26 out of 3,252, or 0·8%, of tests from unvaccinated healthcare workers were positive, compared with four out of 1,989, or 0.2%, of tests from healthcare workers who had a jab at least 12 days before testing.
And when all infections (asymptomatic or symptomatic) were included, the results were just as good:
A marked reduction in infections was also seen when analyses were repeated with inclusion of Health Care Workers testing positive through both the symptomatic and asymptomatic arms of the programme (56/3,282 (1.71%) unvaccinated vs 8/1,997 (0.40%) 12 days post-vaccination, a four fold reduction in overall infection).
This gives overall efficacy of around 80% against all infection.
Astra Zeneca
The best estimate of the Astra Zeneca efficacy against symptomatic infection (with the recommended dosage and interval) is 82%. The same study looks at asymptomatic infection also, and overall efficacy against all infection. The calculated efficacy against asymptomatic infection is around 20% (range of -10% to +45%). And the overall efficacy against infection (with all dosage intervals) is 54% (range of 32% to 70%).
Implications for herd immunity
We keep talking about herd immunity. What does it mean? Herd immunity means that enough of the population are protected (whether by previous infection or immunisation) against a disease that any introduction of the disease can’t get going. In a population without any immunity, any case will spread at its natural rate (for example, for Sars Cov2, before we started taking social distancing actions, this was 2-3 – each person infected on average 2-3 more people, and with the new variants would probably be more like 3-3.5). With a population with some immunity, there is a chance that some of those 3-3.5 people exposed to an infected person will already be immune, so don’t get the disease, and therefore don’t spread it to anyone else. If enough of them are immune, then infectious people have no-one to infect, and the outbreak dies out.
The simple formula for herd immunity is that 1-1/R0. So if R0 is 3-3.5, then 67 – 71% of the population needs to be immune so that any reintroduction of the virus will not keep spreading, but burn itself out. This is important because some people cannot be vaccinated – for example, people with compromised immune systems. So having the whole population immunised protects unimmunised people as well as those who are directly immunised.
In our specific two vaccines, Pfizer is reducing all type of infections (Scenario 3), and Astra Zeneca is mostly only reducing symptomatic infections (Scenario 2). Pfizer reduces all infections by around 80% (compared with 95% for symptomatic infections) whereas Astra Zeneca, reduces overall infections by around 55% (compared with around 80% for symptomatic infections).
Not everyone will be able or willing to be immunised. Let’s assume a campaign can get to 80% of the population. In that case, the impact of a vaccine on herd immunity would be 80% of the efficacy of the vaccine against all infections. So if all of a population was immunised with the Pfizer vaccine (80% times 80% = 64%) the population would probably get to herd immunity or very close to it, but a whole population immunised with the Astra Zeneca vaccine (80% times around 54% = 43%) would probably not get herd immunity. Even if the Astra Zeneca overall effectiveness is at top of the range (70%) the whole population would get to around 56% (80% times 70%) reduction in infection.
For those people who are immunised, either vaccine is great – a massive reduction in symptomatic infection, and even those who have symptoms will have much milder ones. But while the Astra Zeneca vaccine will reduce the spread of SarsCov2, it won’t be enough to stop an outbreak without some kind of social distancing measures.
If Australia opens its borders completely, with most immunised Australians having received the Astra Zeneca vaccine, there will be a very high risk of SarsCov2 continuing to spread, with the potential for non immunised people to get very sick indeed.
A word of caution – these numbers are preliminary, and so there is a wide potential range around them.
Links
In really good news from the UK, the effectiveness of vaccination has started to show up in reduced deaths – this article from the Financial Times has more:
With more than half of the people aged 80 and above having received their first jab by the middle of January, case rates, hospitalisations and deaths in this group of people have started to drop faster than the rest of the population. The effect is small and has only been visible in symptomatic cases since the second week in February. But that accords with the two-to-three week period after the first dose of the vaccine that doctors think is necessary for it to offer significant protection.
And in Israel, with lots more vaccinations, and lockdowns that aren’t as effective, the effect is even more pronounced as this study shows.
After one dose, during days 14 to 20, the vaccine effectiveness was 57% for symptomatic covid-19, 74% for hospitalisation, and 62% for severe disease. The estimated effectiveness in preventing death from covid-19 was 72% in the two to three weeks after the first dose. There was insufficient data to produce an estimate on the reduction in mortality in those who received two doses.
Life Glimpses
In NSW, it is now over 40 days since the last locally acquired case of Covid19 (we continue to have an average of 4 or 5 cases a day from hotel quarantine). And it really is feeling like we are going back to normal. As I’ve said above, working out when to open borders is going to be challenging, but when we have all of our hotel quarantine workers vaccinated, and hopefully their families as well, we can have more confidence in our borders and continue to open up our domestic economy.
My choir is going to meet indoors next week, and this week I met some ex colleagues in a bar (outside, but still with around 20 people). University is at least partially in person for both of my kids. And I’m seriously considering booking a holiday in Western Australia (the state of Australia that has most consistently closed its borders) later this year.
But I still think there is a very slim chance that I’ll be going to Tokyo to watch the Olympics in July, or going anywhere else outside Australia in 2021.
Bit of Beauty
Now that the Northern Beaches are open for everyone in Sydney again, it was lovely to have lunch in Manly recently. A beautiful part of the world.

Thanks Jennifer as always for your thoughts. Right now it feels nations are in a phase of “get an effective vaccine which works as quickly as possible” rather than discussing “which one would be best long-term?”. This question on which can actually achieve herd immunity is interesting and I have a selfish view as we are planning to come back to Australia in January 2022 – hence very interested in your actuarial crystal ball on the likely quarantine situation at that stage for Australians arriving back fully vaccinated …. How will Australia balance keeping COVID low (zero?) against being “open” again?
Finally, I can share with you my on-the-ground Paris culture perspective – increasing rebellion at the long-standing 6pm curfew with minimal policing (judging by the increases in loud weekend parties taking place). However, the Alps were open to French residents (without any ski lifts but with snow, take away cafes and lovely weather), hence my Manly-born kids finally got a big fix of winter sports during February holidays. That had many “bits of beauty” to enjoy in a tough environment here in Europe.
Your comment sounded very positive. Lunch in Manly sounds great. In the evening news on TV, it was announced that the Olympics will take place. Only for local people no visitors. I hope you decide to go to Western Australia.
I understand that the AZ vaccine is proving more efficacious in reality than in trials – do you know anything about that and does it change your view in this blog?
My read is that it is generally better at preventing disease, closer to Pfizer than the original studies (The Economist had a good article recently).