
What proportion of reported Covid19 deaths are caused by Covid19, rather than happening coincidentally? Evidence from here in Australia and also the UK suggests the vast majority of reported Covid19 deaths are caused by Covid, and most other reported Covid19 deaths were hastened by Covid19, even if it was not the underlying cause.
As Australia sadly catches up with the rest of the world, I’m seeing talking points here that I remember reading in 2020 from other countries. The latest is “Not all deaths with COVID are because of COVID”. As the Financial Review reported,
Mr Morrison said there had been 587 deaths in residential aged care this year that were COVID-19 related. At the same time, there had been 4141 total deaths in residential aged care. “When people are passing away with COVID, that does not necessarily mean that they have passed away because of COVID,” he said. “That is the medical advice. That is the health advice.″
What do the statistics suggest? With more than 10% of the population of each of Victoria and NSW having been officially recorded as infected with Covid19 this summer, and the reported Covid19 deaths in January 2022 being around 10% of projected January deaths, it’s certainly plausible that some of the deaths from Covid19 have been co-incidence. But if we look more closely, most reported Covid19 deaths are probably caused by Covid19.
Australia collates daily reports of deaths from Covid19 here, which is summarised in Anthony Macali’s excellent site here, and visualised in the diagram below. These deaths are collated by state health departments, and are counted (as per the COVID-19 national guidelines):
a COVID-19 death is defined for surveillance purposes as a death in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID19 (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death. Where a Coroner’s report is available, these findings are to be observed.
But these daily deaths are not formally certified with a death certificate.
The gold standard for cause of death is a death certificate, where a doctor has certified the cause of death as being Covid19. Death certificates generally take longer to be statistically tabulated, up to six weeks for a doctor certified death, and significantly longer if a death is reported to a coroner. In Australia, the registration system for deaths is state based, so there is an additional delay for information to get from the states to the ABS, which is the statistical body which tabulates the information. This means that compared with many other rich countries, our death reporting is slower. The definition for a death directly due to Covid-19 in these statistics is defined by the WHO:
A death directly due to COVID-19 is defined by the WHO as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death.
The ABS this week put out a new analysis of Covid mortality to the end of January, continuing their efforts to provide much more up to date and seasonal information about mortality compared with pre-pandemic years. This updates a similar analysis they released in December. In the most recent analysis, the ABS reported a total of 2,704 deaths in Australia from Covid19 up to 31 January 2022. There were an additional 148 deaths which had Covid19 mentioned on the death certificate in some way, which were not included in the Covid19 death statistics:
- Covid related but not the underlying cause of death
- A negative Covid 19 result on the death certificate but with some suspicion of Covid
- Deaths with a personal history of Covid
This was around 5% of the total deaths with Covid19 on the death certificate. So 95% of the deaths with Covid19 on the death certificate reported to the ABS by 31 January 2022 were from Covid19. But this analysis is missing around 1,202 deaths compared with the daily reporting. Given that in the last two weeks of January there were 1,059 deaths reported in the daily death count, this difference is most likely to be a delay in death reporting, rather than a difference in which deaths are reported. The most recent deaths are likely to be from Omicron, so we should check the hypothesis that some deaths reported in January were “with” rather than “of” Covid.
There are two ways to do that. The ABS reported twice. Between the most recent two reports from the ABS (as at 31 October and as at 31 January), an additional 885 Covid19 deaths were recorded (some of them had occurred prior to October, but most of them were after) and an additional 75 deaths had Covid19 on the death certificate but which were not regarded as caused by Covid19. In these additional statistics, around 8% of all deaths with Covid19 on the death certificate were not caused by Covid19.
So the Australian evidence suggests that still over 90% of more recent deaths were caused by Covid19.
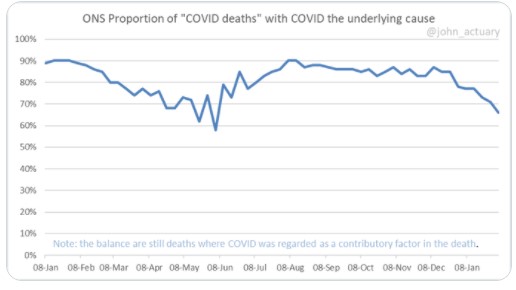
In the UK death certificate reporting is faster than in Australia. There, the Omicron wave has led to an increase in deaths with Covid19 mentioned on the death certificate where the underlying cause was not Covid – from around 10% to around 25% of all deaths.
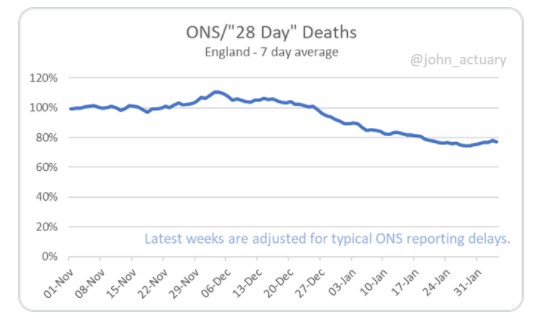
Actuary John Roberts does a weekly analysis. The first graph looks at deaths reported by the Office of National Statistics (ONS) – equivalent to the ABS reporting I have analysed above. In January, the proportion of “Covid deaths” with Covid as the underlying cause has reduced there – from just above 80% to more recently around 70%, and as John points out in the graph, the remaining deaths still have Covid19 as a contributory factor. The second graph looks at the comparison between the UK’s daily reports and the reports based on death certificates.
In the UK, the daily reporting is on a slightly different basis (all deaths within 28 days of a positive test are counted in their initial reporting). By the end of January, where most Covid deaths are probably caused by Omicron, around 80% of all “28 day” deaths are caused by Covid19 (using the final death statistical analysis from the Office of National Statistics). So the UK’s daily Covid19 death reporting would capture more deaths than Australia’s (because they will capture any death with a positive Covid19 test in the month before, whereas Australia’s looks at the probability of Covid19 being the cause).
And even there, 75% of the reported deaths “with” Covid19 turn out to be caused by Covid19.
My conclusion? While some of the deaths may have been coincidence, it seems likely to me that most of them will have been deaths of people who wouldn’t have died at that time if they hadn’t been exposed to Covid19. Many of the other deaths will have been hastened by Covid19 even if the underlying cause was a different illness.
Links
This week I’ve got a few links about Long Covid. First of all a very interesting question from – Nature Magazine Long Covid – why don’t we take it seriously?
From the beginning of this pandemic, people with disabilities understood that the disease would target them and would swell their ranks. Disability historians knew that there was a penumbra of ill health to previous mass-death events. Health economists warned that, as with tuberculosis, HIV and other diseases, morbidity would stalk mortality. Too many others have clung stubbornly to a belief that COVID-19 is something from which a minority of people die, and that most bounce back quickly and intact, with only their immune system updated. The longer the pandemic drags on, the harder it is to maintain that fiction.
A very rigorous study from the US of long term effects of Covid19 on cardiovascular disease over the longer term. The study looked at 159,000 US veterans who survived more than 30 days after contracting Covid19, and compared their cardiovascular disease outcomes with over 5 million matched control patients, and concluded that there is a very significant increase in cardiovascular disease among survivors of Covid19, after 12 months, which is worse the more severe the initial Covid19 disease..
We show that, beyond the first 30 days after infection, individuals with COVID-19 are at increased risk of incident cardiovascular disease spanning several categories, including cerebrovascular disorders, dysrhythmias, ischemic and non-ischemic heart disease, pericarditis, myocarditis, heart failure and thromboembolic disease. These risks and burdens were evident even among individuals who were not hospitalized during the acute phase of the infection and increased in a graded fashion according to the care setting during the acute phase (non-hospitalized, hospitalized and admitted to intensive care). Our results provide evidence that the risk and 1-year burden of cardiovascular disease in survivors of acute COVID-19 are substantial. Care pathways of those surviving the acute episode of COVID-19 should include attention to cardiovascular health and disease.
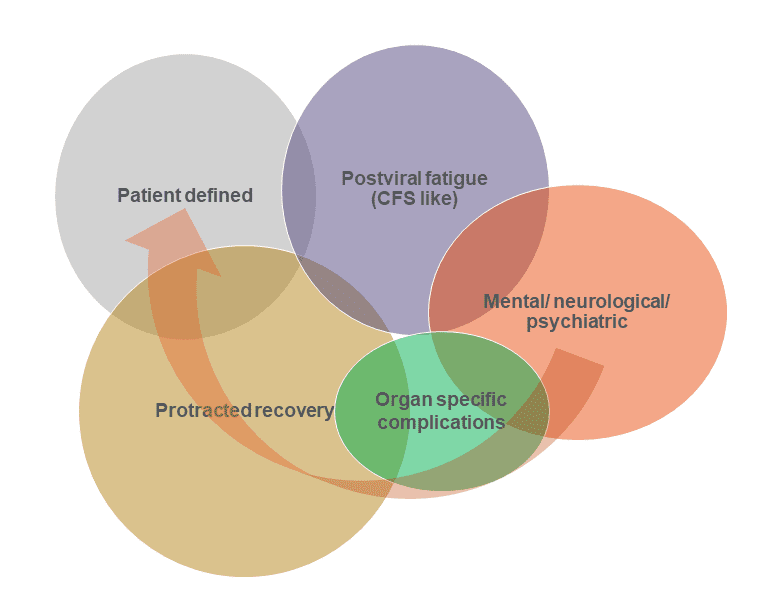
And this summary article from Dr Achim Regenauer, looks at the implications of Long Covid for life and health insurers, and concludes that it is likely to involve a number of different causes:
Three recent studies, however, stand out to me as having enhanced our understanding. It’s these, and the conclusions we can potentially draw from them, that have led me to consider that there are possibly five long Covid subgroups; see the diagram. In addition, with close to half of the COVID-19 patients in these studies (with variation by study) still reporting symptoms after a year, there are obvious and significant consequences for Life & Health insurers.
In news that will surprise no-one who had any contact with a workplace in January in Australia, there was a dramatic increase in the number of people not working due to illness. The ABS’s most recent report into hours worked showed 3.4% of the workforce was away from work for a whole week in January, with NSW and Victoria having a 13.5% reduction in hours worked compared with a normal January.
“January is the middle of summer and usually only around 90,000 to 100,000 people in Australia are away from work sick for an entire week. In January 2022 it was around 450,000 people (3.4% of employed people),” Mr Jarvis said. “The January 2022 figures are also much higher than in the winter months in Australia, when sick leave has usually peaked in August at around 140,000 to 170,000 people.”
Life Glimpses
In NSW we continue to have thousands of cases of Covid a day, but most restrictions (except mask wearing) have gone – it’s all about personal responsibility now. So any gathering continues to be a cautious (and sometimes awkward) comparison of risk appetites – whether to meet inside or outside, what about asking people to do a rapid antigen test first, etc etc.
One of our kids hosted a party this month of about 20 people (which would have seemed a small number a few years ago, now seems enormous!), and asked all the guests to do tests first. We had to supply some of the tests (as they are still not easy to find). I remember back in December reading someone in the US describing asking this of their guests, which seemed an incredible thing before a party. But now, here in February in Sydney, all of the guests were very happy to comply and we had drinks and snacks set up outside for the people waiting the 15 minutes for their test results. So far, a week later nobody appears to have brought COVID to the party, which is a relief.
Bit of beauty
It doesn’t belong here, but I found this beautiful thistle on a walk around the lake in Canberra. One for my NZ cousins to admire.

There’s another category of covid-related deaths: those that didn’t catch it. I hear stories from hospital of delayed treatment (eg surgery) due to covid constraints, that resulted in death.
A doctor friend tells me that we are short about 100,000 cancer diagnoses, 10k for breast cancer alone. That means ten thousand women are walking around with a breast cancer that they would have known about in normal times.
Agree, Tim. We don’t have all the statistics about deaths in Australia (only Covid) over the summer, so we can’t tell whether other deaths (from delayed or unavailable treatment) are higher than normal. And some of the treatment delays will have effects later than this summer.
Jennifer, good analysis as always. On question I’d raise is what our acceptance threshold is for a disease like COVID. I know you aren’t implying it should be zero, however we have treated this disease with a very low threshold because we believed this would avoid an unacceptable level of death.
Now that we are years into this disease, I think it is important that we recalibrate our perspective that minimisation of harm and death is the objective, not eradication.