
Insight
The possibility of reopening schools in Term 2 continues to be debated in the press (and here at home). As I mentioned in my last post, here in NSW, Gladys Berejiklian announced that schools would reopen to students in the third week of Term 2 (that’s May 11 – in three weeks). That followed Scott Morrison a few days ago pleading with teachers to allow schools to stay open.
Different countries are dealing with this issue in different ways, but almost every western country has had some form of school closure by now. And some are starting to open back up again. So I wondered what you have to believe to reopen schools? It seems to me there are two key assumptions you have to believe to reopen schools, even with reasonable social distancing.
- Children are not at serious risk from Covid 19 – This seems a reasonable assumption
- Allowing children to see each other will not increase the spread of Covid19 between children (and hence back to their families) or to their teachers. I’m not convinced by this one, although I haven’t been able to find anything that directly studies this question
Risk to children from Covid19
There are now quite a few sources of case fatality rates by age. All of them suggest that the risk of death to those under 20 is very low. The deaths in this age group are rare enough that they make international headlines. So it does seem reasonable to think that children are unlikely to die from catching Covid19 at school (they could have an unpleasant illness, but they are very likely to recover).
Can children spread the disease?
This is the key question. And the short answer is we don’t know. But based on everything I’ve read, I would suggest yes, they can, but just not as much as adults.
There are two underlying questions here. Do children get infected, but without symptoms? And if they do get asymptomatic infection, can they spread the disease to others? The limited information we do have suggests that children do get infected, but not as much as adults, and that when they are infected without symptoms, just like adults, they can transmit the disease, but not as much as somebody with symptoms.
In my search for answers, I started in Iceland, which is carrying out the closest thing to randomised testing that I have seen. It is not random – it relies on volunteers to turn up and be tested, but they are people without symptoms. This paper analyses what they have found to date.
To complement this testing [testing of symptomatic individuals] and provide a view of the spread of the virus in the general population, on March 13 deCODE began testing volunteers who signed up for free screening. By April 1, 10,797 people had been screened in this effort, with 87 (0.8%) testing positive. From April 1 to April 4, an additional 2,283 randomly selected individuals were screened, with 13 (0.6%) testing positive. Analysis of the combined testing data suggests that children and women are, in general, somewhat less susceptible to SARS-Cov-2 infection than men and adults.
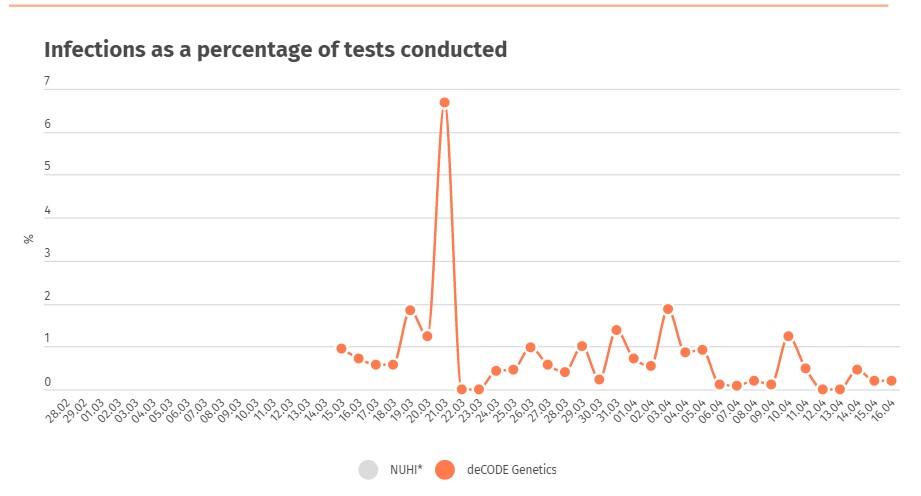
Looking at the Icelandic summary website today (18 April), the random testing has resulted in an overall positive rate over the past month overall of 0.7% – so 0.7% of the Icelandic population tested positive for Sars-Cov-2 despite having no symptoms. Overall around 10% of the positive tests are for children whether symptomatic or not (those 18 or under) while around 25% of the population is under 18.
But we don’t know what proportion of the asymptomatic positive tests were children.
And we also know that asymptomatic carriers do exist – either because they haven’t had symptoms yet, or their symptoms are so mild that they don’t notice them. The best completely controlled population we have is the Diamond Princess (the one that was marooned off Japan in January/ February). This study shows that around half of all positive tests on that ship were asymptomatic (328 out of 634). And this study of a small town in Italy (Vo) suggests an even higher percentage of asymptomatic cases – around 70%.
The two major pieces of modelling I’ve looked at that model likely spread of the disease have made fairly similar assumptions about children. The Imperial college modelling in the UK from mid March concluded that closing schools would help to suppress transmission of the epidemic, but wouldn’t be enough on its own.
We predict that school and university closure will have an impact on the epidemic, under the assumption that children do transmit as much as adults, even if they rarely experience severe disease. We find that school and university closure is a more effective strategy to support epidemic suppression than mitigation; when combined with population-wide social distancing, the effect of school closure is to further amplify the breaking of social contacts between households, and thus suppress transmission. However, school closure is predicted to be insufficient to mitigate (never mind suppress) an epidemic in isolation; this contrasts with the situation in seasonal influenza epidemics, where children are the key drivers of transmission due to adults having higher immunity levels.
The Sydney University modelling in early April used explicit assumptions about children, which were set to replicate as closely as possible the actual experience of the disease in Wuhan.
The fraction of symptomatic cases was set to two-thirds of the total cases (σ = 0.669), which concurs with the modelling study of Ferguson et al. [26]. However, we found that the best calibration is achieved when this fraction is age-dependent, with the fraction of symptomatic cases among children calibrated to one-fifth of the one for adults, that is, σc = 0.134 for children, and σa = 0.669 for adults. This calibration outcome per se is in agreement with the reported low attack rates in children worldwide, and the observation
that “children are at similar risk of infection as the general population, though less likely to have severe symptoms” [38]. Another study of epidemiological characteristics of 2,143 pediatric patients in China noted that over 90% of patients were asymptomatic, mild, or moderate cases [39]. In our study, the attack rates in children have converged to 6%, as shown in Figure 2, that is, only 6% of infections are detected in children, even with a relatively high reproductive number R0 = 2.27 and a relatively long generation period of 6.4 days (in comparison, the generation period for influenza varies in AceMod in the range from 3.35 to 3.39 days).
I’m not sure if I fully understand all of that paragraph! But my interpretation is that children are much more likely to be asymptomatic than adults, if they catch the disease (only 20% of the symptoms of adults). But the Sydney University study concluded that school closures were not that useful an intervention – they delayed the peak by 2 weeks, but other interventions were more useful.
So reading all of that research my view is that we don’t know enough to reopen the schools while there is still Covid19 in the community – the risks are unknown, and it isn’t an easy decision to reverse.
But just as a final point, one of the biggest clusters of cases in New Zealand was, you guessed it, a school.
It’s been a nightmare four weeks for the students, staff, and parents of Marist Girls’ College in Auckland. The school’s COVID-19 cluster currently sits at 92 cases, but the good news is 79 of those have recovered.
It’s unknown how the virus got into the school, and its spread put the spotlight on testing criteria in New Zealand. After the college was deemed a cluster, calls were made for all New Zealanders showing symptoms to be eligible for a test.
Late last month, Prime Minister Jacinda Ardern announced exactly that – criteria was widened so “anyone” with symptoms of the virus could be tested.
One of those from Marist College who tested positive for COVID-19 was principal Raechelle Taulu. She has since recovered, and says she’s now focused on helping her school reopen.
I do sometimes wonder why the Australian media doesn’t seem to notice what happens in New Zealand unless Australians are involved.
Link
This fascinating link is about cholera riots in the 19th century – and how the level of support given to those suffering the most from the various quarantine regulations imposed on the population led to different outcomes in terms of level of public support or lack of it in the form of rioting.
As a pandemic swept through Europe in 1831, a riot broke out in Königsberg. “Groups of people who did not agree with the cholera regulations assembled [on July 28] for the funeral of a journeyman carpenter,” the Prussian State Gazette reported. After refusing a request to disperse, the dissenters “invaded the Police building and threw files and papers into the street. The military fired on the crowd and eight people were killed.” The newspaper attributed the revolt to “a general misunderstanding of the interpretation of the measures against the cholera.”…Similar cholera riots broke out across Europe that year, and still more erupted periodically for decades afterward. …
The more high-handed the ruling classes were, the more likely they were to be targeted by rumors and revolt. The riots persisted longest, Cohn writes, “where elites continued to belittle the supposed ‘superstitions’ of villagers, minorities, and the poor, violated their burial customs and religious beliefs, and imposed stringent anti-cholera regulations even after most of them had been proven to be ineffectual. Moreover, ruling elites in these places addressed popular resistance with military force and brutal repression. By contrast, distrust and rumours of purposeful poisoning abated where elite attitudes and impositions changed.” …
As Königsberg and other Prussian cities were rioting in 1831, the authorities in Berlin loosened the local cholera regulations; the government and middle-class charities also organized relief efforts. Berlin did not riot.
As various parts of the US seem to be going down the same path as Königsberg in 1831, it is a good reminder that it is probably not a coincidence that the US is starting from a position of the lowest support for those suffering from lockdowns and shelter in place orders (to say nothing of the level of healthcare available to those who have lost jobs there).
Life Glimpses
In support of our continuing quest for the perfect cupcake, this week I combined my bike ride with a trip to a cooking supplies shop (it is mostly a wholesaler, but if retail customers turn up they will sell to you). I realised when I got there that this is the first time I’ve physically bought something for about a month – I’m not the designated shopper in this house. Although, given it was a wholesaler, I was the only customer, and there was hand sanitiser everywhere, so I felt quite safe.
Probably just as well I rode my bike there – we have a very well set up kitchen, and we don’t cook anything very sophisticated, but I always want to buy the cool gadgets in a shop like that. My bike panniers don’t hold all that much though – just the piping bags that I had been sent out to get.
Bit of Beauty
Today’s picture comes from the glorious evening yesterday in Sydney. The light was that perfect pre sunset light that sometimes happens after a clear day in Sydney.

I wholly approve the quest for the perfect cupcake. Hopefully whenever we will meet,
I will be able to enjoy the fruit of your labour. Keep it up. The photo looks like a painting,
you could enlarge it to a poster size.
The Insight part of your reflections is far too professional for me to comment.
Love. Marta
A fantastic summary of the school situation thanks Jennifer. Every time I read something new about schools I change my mind about whether I agree to them being open or not. I wish our politicians would clearly articulate the evidence for and against rather than just saying “based on medical advice”. It gives me no confidence in the decision making.
Another interesting piece of information in relation to schools is contained in the NSW Health press releases from 2 April to 9 April. Mentions of lots of cases where teachers/students have been diagnosed.
Thank you for identifying the critical question re the risk of schools re-opening ie What is the probability that children will increase the spread of Covid19 between children (and hence back to their families) or to their teachers? Depending on the day, I am amazed/disappointed/frustrated that no effort seems to have been made to answer this important question which is the subject of great debate and which affects literally millions of Australians. You are probably tired of me suggesting random tests so let’s say that they are too hard for some reason. We do know that the period for rapid growth in known cases was in the 2nd half of March when schools were mostly open. Using NSW data, the known cases increased from 210 (17 March) to 2182 (31 March). Surely the contact tracing records can provide some facts on the extent of actual transmission via the NSW school system? If the transmissions were minimal during the “laissez-faire” period then surely the current risk will also be low? Alternatively, if it was common then we shouldn’t be re-opening schools without further investigation (like random testing).
Good idea Martin, you and I should also check out Karen’s info from NSW Health. I never tire of people suggesting random tests, I think we should be doing it! Also, check out Iceland – they are testing the population at large there (not quite randomly).
I did have a look at your link to Iceland’s semi-random testing results. I don’t think it is coincidence that they have planned relaxation of specific measures on 4 May: https://www.garda.com/crisis24/news-alerts/332531/iceland-covid-19-restrictions-to-be-relaxed-on-may-4-update-2
In my spare time this evening I discovered that a genuine random testing study began in Slovenia today. Here is the newspaper report: http://www.sloveniatimes.com/comprehensive-random-testing-for-covid-19-starts-today
Interesting design (with a population of around 2 million). I am keen to find out how many “volunteers” take the test. I hope that the results are publicly available. I will do a search next week.
Just an fyi from UK: https://www.medrxiv.org/content/10.1101/2020.04.07.20052340v1