
The Omicron Variant is spreading fast around the world. All the evidence is pointing to higher infectiousness, and less effectiveness of vaccines. It is still not clear whether the disease is less severe. But even a less severe variant is still bad news.
Here in Australia, already nearly 5% of cases being sequenced are Omicron (rather than Delta) and NSW is back to rapidly increasing case numbers after staying consistently around 200 cases a day for the last couple of months. We’ve even got a few superspreader events in the news, including a nightclub cluster with 84 cases.
So what do we know?
- Transmissibility – all the evidence is pointing to faster/better transmission – I’ve read analyses suggesting spread of between two and four times as fast as Delta
- Effectiveness of vaccines and previous infections – lab studies, and to a lesser extent real world analysis, suggest that both vaccines and previous infections are much less effective against Omicron than previous variants, but again, in these early stages, it is very hard to tell in the real world.
- Severity of disease – much harder to work out what we know here, because severe disease and death take a while to develop in all varieties of Covid, and given how variable rates are already by age and vaccination status, it is really important to compare like with like.
The UK Actuaries have a great summary here.
What are the implications? This is reminding me of when I first looked at the Alpha variant nearly a year ago. Fundamentally, unless the new variant is not dangerous at all, a more infectious variant is still bad for all of us, even if it less dangerous. What scares me about Covid19, now that I’m vaccinated, is Long Covid. So I’ve built a little thought experiment of Delta and Omicron. Right now in Australia, with current public health measures and high vaccination it seems that we are keeping Reff to about 1, with just the Delta variant. But NSW’s spread is taking off, at the same time as the Omicron variant is seeding various superspreading nightclub events. So what if you are half as likely to get Long Covid with Omicron (1% chance, instead of 2% with Delta), but Omicron spreads at a rate of growth of 10% a day instead of staying stable? Here’s what the graph looks like.
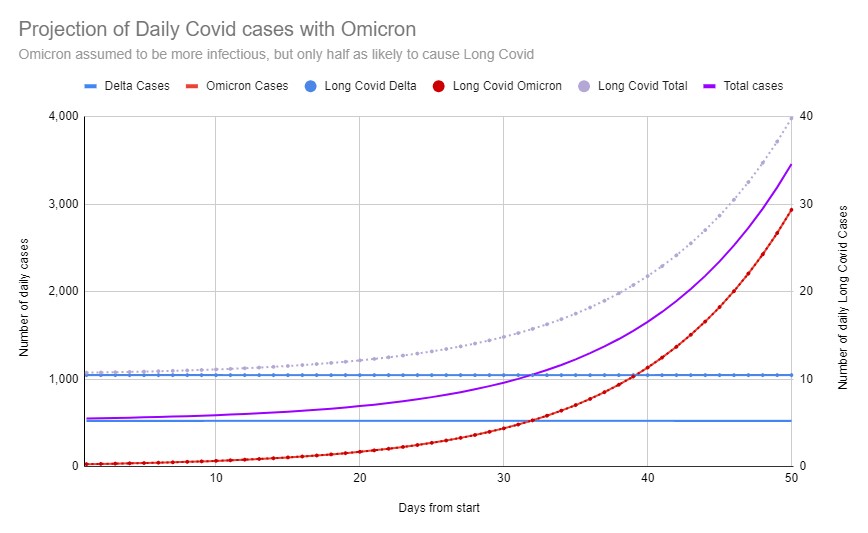
This graph illustrates that if it increases the chance of everyone catching it, a milder disease can be still be more dangerous. The Delta cases – both Covid cases, and Long Covid cases – stay stable every day. But the Omicron cases, despite starting at only 5% of the total, end up quickly overwhelming the less infectious Delta cases. While only half as many people with Omicron end up with Long Covid (as those who catch Delta), nearly twice as many people in total still end up with Long Covid after 50 days, once Omicron gets into the population, as so many more people catch the disease.
So what should we do?
- Vaccination – get a booster if you can, as the evidence strongly suggests that boosters protect much better than initial doses against Omicron (I’m assuming anyone reading this blog will already be vaccinated).
- I’m continuing to try and socialise in well ventilated settings, like outdoor restaurants, when I do go out, rather than small crowded indoor venues. And I’m considering upgrading my masks from the basic fabric ones I normally use, for high risk settings as cases increase here in Sydney.
- Public health – We should be keeping our current public health settings in play – QR codes in all shops and venues, masks in indoor settings.
- And at a national level, we should be supporting Covax – vaccinating the world, not just ourselves. This variant probably arose somewhere in Africa, where population level vaccination is very low (12% of the population has had at least one dose). Fixing that takes vaccine doses, and funding for strong, supportive public health actions to outweigh the anti vaccination propaganda. In our region, Australia should be doing far more to support Papua New Guinea. Not just providing vaccines, but providing logistical and public health support for a complex country where vaccination of all types is very challenging.
Links
The UK Actuarial Response group has developed a rigorous framework for estimating the Quality Adjusted Years of Life Lost (QALYs) from Covid19 here. It’s very useful to understand the cost of the disease in not just deaths, but disability both short term and long term.
Our objective was to develop the framework, as we recognised quickly that understanding of the disease would advance significantly both while we were developing the model, and ahead of the publication of the paper. Indeed we had to update the parameters used in the model several times during the course of the project, as better information on the longer term consequences of COVID-19 became available.
The model quantifies morbidity impacts from acute COVID-19 illness, as well as the impact on those who suffer from ongoing Long-COVID symptoms for several weeks. Lastly, it includes those who are permanently injured as a result of their illness or treatment, for example some of those who survive intensive care.
It is the framework that is the main output of our modelling, as opposed to the results that we obtained using a particular set of assumptions. Nonetheless, our modelling gives an indication of how significant the burden of disease may be.
Assuming that 3 out of 5 people in the UK become infected, we modelled 300,000 QALYs lost within one year of infection and 558,000 lost within ten years. The usual UK Government estimates of willingness-to-pay to avoid these QALY losses would be up to £17.9 billion and £32.2 billion, respectively.
This story is a bit older, but useful as a reminder that testing and isolation is very important in controlling this disease. This summary from the Economist describes the situation. A study in the UK looked at the effect of an error in a COVID19 testing lab which resulted in thousands of positive test results not being reported back to those tested.
The agency said that the firm had incorrectly told 43,000 infected people that they were virus-free. The cause of the error remains unclear.
That in turn meant that those people didn’t isolate, and then infected others. The paper estimated the impact, partly by looking at the local areas involved and the greater increase in cases compared with areas where the error did not occur:
…each faulty test may have led to 0.6-1.6 extra cases (the range reflects uncertainty over how many people who tested positive received earlier false negatives). Based on Britain’s case-fatality rate, this translates to 100-250 deaths.
There are a few lessons from this story:
- every chain of the testing process matters – its not just getting the test performed, but communicating it
- And the value of self isolation is shown by the difference between places where communication happened and it didn’t. The Doherty report emphasised test trace isolation quarantine in their modelling for very good reason.
Life Glimpses
Sydney, where I am, is still only open for the fully vaccinated (if you are over 16). According to the statistics on 10 December, there are just over 450,000 over 16s in NSW – 6.9% of them – who are not yet fully vaccinated, and around 100,000 of them have had a first dose. So there aren’t that many people under lock down here in Sydney any more.
It has been great going out and about once more, catching up with people in cafes, restaurants, a play, and even a conference of more than 200 people! And at the Circular Quay end of Sydney this week, there were people everywhere, enjoying themselves. This is the peak party time of the year here in Sydney, and we are all taking advantage of it.
I’m quite conflicted about whether I want further restrictions with this new wave. While I think it would be sensible, I’m hoping that they don’t come in until after I have seen Hamilton (I’m onto my third booking, which is this week, and I have high hopes I will be able to go).
Bit of Beauty
Now that we’ve got a bit more sophisticated in our cocktail palette in the ActuarialEye family, we went out to try cocktails made by professionals. They certainly looked fantastic, as you can see in the picture (and were pretty tasty too).

Good analysis and good suggestions. Is the chance of long covid (in Australia) changed by the availability of the new anti-viral treatments?
How long do you think it will be until we get an Omicron-specific booster?
Can you share with me the name of the
cocktail, it does look pretty and as you say
tasty too. Thanks.
One swallow doesn’t make a summer, but we can see the Mission at Capistrano from here:
https://twitter.com/CrocodileChuck/status/1473516128949309444
I found this article very interesting, thanks for sharing