
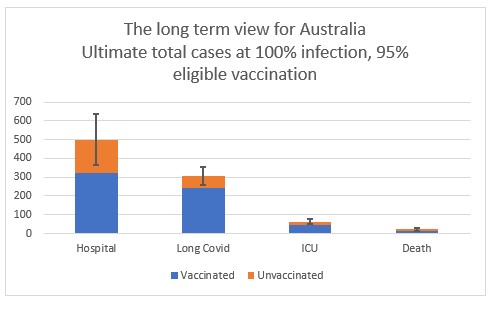
If everyone in Australia who can be vaccinated, is vaccinated, what can we expect when Covid19 becomes widespread in the population? If, after everyone in Australia who can be is vaccinated (I’ve assumed 95% of everyone 12 and over), everyone in Australia is exposed to Covid19, what can we expect from Covid19? There are likely to still be significant pressures on the hospital system, particularly if it happens too quickly.
We can expect around 400,000 – 600,000 eventual hospitalisations (60% of whom would have been vaccinated), with around 50,000 – 80,000 (70% of whom would have been vaccinated) of those ending up in ICU. Around 200,000 – 400,000 people are likely to end up with Long Covid, the majority of whom (150,000 – 250,000) will be of working age. And around 15,000 – 25,000 (50% of whom would have been vaccinated) deaths from Covid are likely to occur. How long will that take? That depends on how well we control the spread of Covid19.
 Simplistically, this involves looking at the total population, assuming they all catch Covid19, and the vaccines are effective. This won’t happen all at once; but it seems likely to happen eventually. And if you’re surprised by how high those numbers are, its because Covid19 is a terrible disease – current studies estimate that Pfizer and Astra Zeneca both prevent just over 90% of deaths, but sadly, not 100%.
Simplistically, this involves looking at the total population, assuming they all catch Covid19, and the vaccines are effective. This won’t happen all at once; but it seems likely to happen eventually. And if you’re surprised by how high those numbers are, its because Covid19 is a terrible disease – current studies estimate that Pfizer and Astra Zeneca both prevent just over 90% of deaths, but sadly, not 100%.
If all that happens in 12 months, then we will need around 5% of our total hospital capacity for Covid19 cases that year, and Covid19 cases will take up around 60% of our ICU capacity. And Australia’s death rate in those 12 months will be around 10-15% higher than a normal year.
The current ICU capacity could not cope with 60% occupation from Covid19 cases. The weekly report on Covid19 in Australia shows red if we get to 30% of ICUs with Covid19 cases, and the action is to borrow capacity from other parts of Australia. Even the hospital system would probably struggle – at its peak NSW in its current wave didn’t have as many people hospitalised as the 12 months burden would imply. If we could space this out for longer than 12 months, then the burden on our ICU system in particular, and hospital system in general would not be as great.
At some point, we are going to be living with Covid, even after full vaccination. To be ready for that, these numbers suggest that:
- We have to keep flattening the curve, so that our ICU system can cope, even after everyone is vaccinated – that looks like some degree of continuation of social distancing, mask wearing, contact tracing and isolation.
- We have to invest in our hospital system (including the people in it) right now, for the long term, as it’s not clear how many repeat cases of Covid19 there will be even after everyone has been infected once.
- With around 300,000 people projected to live with Long Covid (200,000 of working age) it is important to significantly invest in appropriate treatments and supports so that those people can be as much part of normal life (including working life) as possible.
I’ve used assumptions from a variety of sources to get to these calculations:
- 95% of the eligible population is vaccinated – leading to 81% of the total population vaccinated (no under 12s). If this gets to 100%, the picture looks better.
- Vaccine effectiveness against symptomatic disease, hospitalisation and death from the assumptions used by the Doherty modelling
- A split of 50/50 Pfizer and Astra Zeneca (this assumption doesn’t make much difference, as they are close to equally effective against severe disease and death)
- Hospitalisation rates based on NSW Health hospitalisations for the current wave up to mid September, which means I might be double counting a little bit of vaccine effectiveness.
- Hospitalisation durations based on the underlying source epidemiological work for the Doherty modelling (10 days for non ICU cases, 15 days for ICU cases)
- Death rates from a worldwide investigation based on serological studies published in Nature (which is possibly optimistic, given some evidence suggests Delta has higher death rates)
- Long Covid rates are the hardest to find – there is a wide variety of outcomes depending on how it is defined and how the study is performed. I have assumed 10% of all symptomatic cases end up with long Covid (and using assumptions about reductions in symptomatic Covid after vaccination from the Doherty modelling to get to those cases). I’ve assumed only 2% of symptomatic cases in children end up with Long Covid.
Links
This actuarial article looks at the game theory of immunisation incentives, suggesting that positive incentives are better than negative ones.
This shows that current policies for providing positive incentives (such as easier overseas travel and access to certain events) for vaccinated individuals will result in a better outcome for society as a whole. The incentives should be strong enough to limit the size of the group refusing the vaccine to the extent that this group’s choice does not impact the outcome of society as a whole.
Rethinking herd immunity at a local level – this article about the US cautions that responding to Covid19 based on population level measures is likely to miss impacts of local community level impacts.
A detailed understanding of local pandemic conditions is necessary to create focused, tailored responses. While achieving high levels of vaccination is important, exclusive focus on national vaccine targets de-emphasizes the complexities of Covid-19 population immunity. Herd immunity is dynamic and depends on the transmissibility of each new Covid-19 strain, the effectiveness of previous immunity due to previous infection and vaccination against these strains, and human behavior in local communities.
And a typically thoughtful article on public health and how it depends on many unexpected things from Tim Harford, shows the importance of community and a safe neighbourhood.
The CDC analysis had compared pairs of individuals, contrasting those who had died with apparently similar individuals who had not. Klinenberg compared two adjacent Chicago neighbourhoods: North Lawndale and South Lawndale. North Lawndale had a heatwave death rate 10 times higher than South Lawndale. Why? Both neighbourhoods had plenty of poor elderly people living alone and both were overwhelmingly non-white. But in other ways they were different.
North Lawndale was depopulated, an urban desert with vacant lots. Gangs used it as a convenient place to sell drugs. “We used to sit outside all night and just talk,” said one resident. But with bullets flying, that became impossible. Big employers such as International Harvester, Sears Roebuck and Western Electric had moved away and shops had closed. People didn’t leave their apartments because they were afraid of being mugged or burgled. They weren’t used to walking to local shops — and there weren’t many local shops to walk to.
South Lawndale, by contrast, was overcrowded, but as a result it felt bustling — and safe. (The area is now known as “Little Village”.) You could step outside your door any time and there would be folk around. When the heatwave struck, elderly residents were happy to walk into an air-conditioned store nearby and hang out. They felt safe leaving an empty apartment behind. When at home they felt safe opening their doors to the people who came to check on them. In a heatwave, lively streets save lives.
Life Glimpses
Last year’s lockdown had our household on a quest for the perfect cupcake. This year, with everyone in the house now over 18, we’ve switched to a quest for the perfect cocktail. It’s been a fun journey, even though I feel as if we are 12 months behind everyone else I know. This week I learned how to make a lemon twist (with the internet’s aid of course) which is probably a life skill I should have had by now.
 As NSW inches towards the next stage of our opening roadmap (70% of the adult population double vaccinated, or 56% of the total population) we’ve realised we need to start practising how to ask people whether they are vaccinated. Most of the new activities (for example having people in your own house, or a group of up to 20 people outside) are only available to those who are fully vaccinated. This explainer points out that the simplest way to start the conversation is by offering your own vaccination status first. My own local area has gone from one of the most vaccinated to the least vaccinated in Sydney (probably because we haven’t had that many cases, so people have been a bit apathetic about it) so I probably need to get used to that conversation.
As NSW inches towards the next stage of our opening roadmap (70% of the adult population double vaccinated, or 56% of the total population) we’ve realised we need to start practising how to ask people whether they are vaccinated. Most of the new activities (for example having people in your own house, or a group of up to 20 people outside) are only available to those who are fully vaccinated. This explainer points out that the simplest way to start the conversation is by offering your own vaccination status first. My own local area has gone from one of the most vaccinated to the least vaccinated in Sydney (probably because we haven’t had that many cases, so people have been a bit apathetic about it) so I probably need to get used to that conversation.
This weekend is the last weekend of the current lockdown in Sydney, at least for those who are fully vaccinated. And just in time, I’ve finished my tour of the boundaries of my local government area – North Sydney Council – on foot and by bike. Even though my local government area is so small that 5km from my house was further than the boundary in every direction, it was fun to see exactly where the boundaries were, and notice the street signs change. The water boundaries are, of course, the most picturesque.
Bit of beauty
Part of our quest for the perfect cocktails is my bit of beauty today – a White Lady.

Thanks, Jennifer.
I have a working assumption (drawn out of thin air) that 20% of the population will be exposed to Covid19 infection every year – which would take your deaths down to an annual rate of 3,000 – 5,000.
This is 5 to 8 times the average annual total of flu deaths, for which vaccination coverage and efficacy are both much lower. So, intuitively, it feels a little high to me.
Nevertheless, I think that we’re looking at a minimum of 1,000 to 2,000 Covid19 deaths in a typical year, so there’s still plenty to be gained from targeted defence measures (e.g. air travel, aged care and hospitals) and further development of treatments, vaccines and vaccine alternatives. All the more so if Long Covid really does turn out to be a long-term debilitation.
Just out of interest, how do the numbers change if the vaccination rate is lifted and/or a percentage of the under 12s are also assumed to be vaccinated? And is the model nuanced enough to reflect higher vaccination rates among the most vulnerable?
Thanks Richard. I agree that vaccination coverage and efficacy are much lower than for flu, but the disease itself is much worse. And I agree that my 100% of population feels over the top, even with no defence measures, but I think we need quite a few defence measures (like a general move outdoors, good ventilation indoors wherever possible, and a change in behaviour to stay home when you are sick0 to get down to 20% a year.
The model is not nuanced enough to reflect higher vaccination rates among the most vulnerable (it is purely aged based on outcomes, and 95% for all age groups over 12). If we get to 100% over 12s, deaths halve, but hospitalisations only decrease by 25%. And if under 12s are vaccinated, it hospitalisations do reduce, but there will still be pressure on the hospital system in my 12 month scenario.
As usual I cannot comment on the serious data.
Went to my first subscription concert this season. The place was full (2,500 seats), everybody having a mask all the time. The concert was great, the soloist Joshua Bell, violin.
Like the name of the cocktail, White Lady, very noble. I seem to recall there is also White Lady Funerals !! am I right. love
The other positive thing regarding slowing down is that treatments are getting better too, and hopefully this might reduce hospitalisation and deaths as time goes on (or is that now termed ‘moving forward’) .
Yes there is White Lady funerals. Perhaps this is what they all have at the end of each day! Looks and sounds inviting.
So we may never get to 95% of people exposed to covid.
What vaccination rate would it take to get R-eff below 1? I’d have though that 95% would do it. Assume that there is still testing and isolation of infectious cases. Even without contract tracing, close contacts are easy enough to identify.
NSW case counts have been declining during a lockdown that is fairly lax, and the vax rate is still rising.
I reckon that there will be some longer-term behaviour changes too. Eg today some people in the street were wearing masks when they didn’t have to.
According to the Doherty report (I blogged about this here) 80% over 16 vaccination reduces the Reff by 2.3 (from a Delta Reff of around 6.0).They don’t look at 95%, but each extra 10% seems to give another 0.2 or 0.3, so let’s say 95% would be a reduction of around 3.0. That means we would still need a combination of effective Test trace isolate and quarantine and the kind of public health measures we had before our current lockdown (checkins, masks on public transport, more working from home) to get the Reff below 1. I hope there will be more behaviour changes too – particularly people not going to work when they are sick, which is hard to imagine now.